

The public wants Governors to reduce Medicaid administrative burdens as the Public Health Emergency ends
A national survey shows broad support for states to do more to protect Medicaid enrollees


The Public Health Emergency is officially ending this spring. This might seem like an official acknowledgment of a return to some sort of normalcy. But look into the details, and a catastrophe is looming. An estimated 7 million Medicaid recipients will lose coverage despite continuing to be eligible. However, states have a number of policy tools at their disposal to limit coverage losses. As two public policy scholars, we undertook a national survey to understand what the public is thinking about this, and found broad and bipartisan support for state governments to take aggressive steps to ensure that eligible Medicaid recipients maintain coverage.
To understand the problem requires understanding what the PHE is, and what will happen when it lapses. The Trump administration initiated and the Biden administration continued PHE declarations to allow states to access more resources to ensure high health care coverage during the pandemic. In return for more money, states could not limit eligibility or add “more restrictive methodologies or procedures.” These policies contributed to a 30 percent increase in Medicaid enrollment.
When the PHE ends, Medicaid enrollee will have to start filling out forms they have not seen in years. Addresses may be outdated. State officials will be overwhelmed. Governors could also decide to make enrollment processes even more burdensome, by add confusing paperwork or documentation requirements. Such requirements matter to take-up. For example, a recent study of the pre-pandemic trend of children losing health insurance found that "increased administrative burdens placed on families reduced public health insurance coverage by a mean of 5.4 percent within the year following the implementation of these changes."
The end of the PHE will create short-term and long-term problems for Medicaid coverage. In the short run there will be an immediate massive loss of Medicaid coverage. In the longer run, to the extent that states lapse back into old habits of making access to Medicaid more onerous, fewer people will access public health insurance.
To inform this discussion, we did something unusual: we asked people about administrative processes. We fielded a nationally representative survey of just over 4,000 people to ask people about specific administrative actions that states could take to protect Medicaid enrollees as the PHE ends. (The paper is forthcoming in Health Affairs: Scholar and an open access version can be found here).
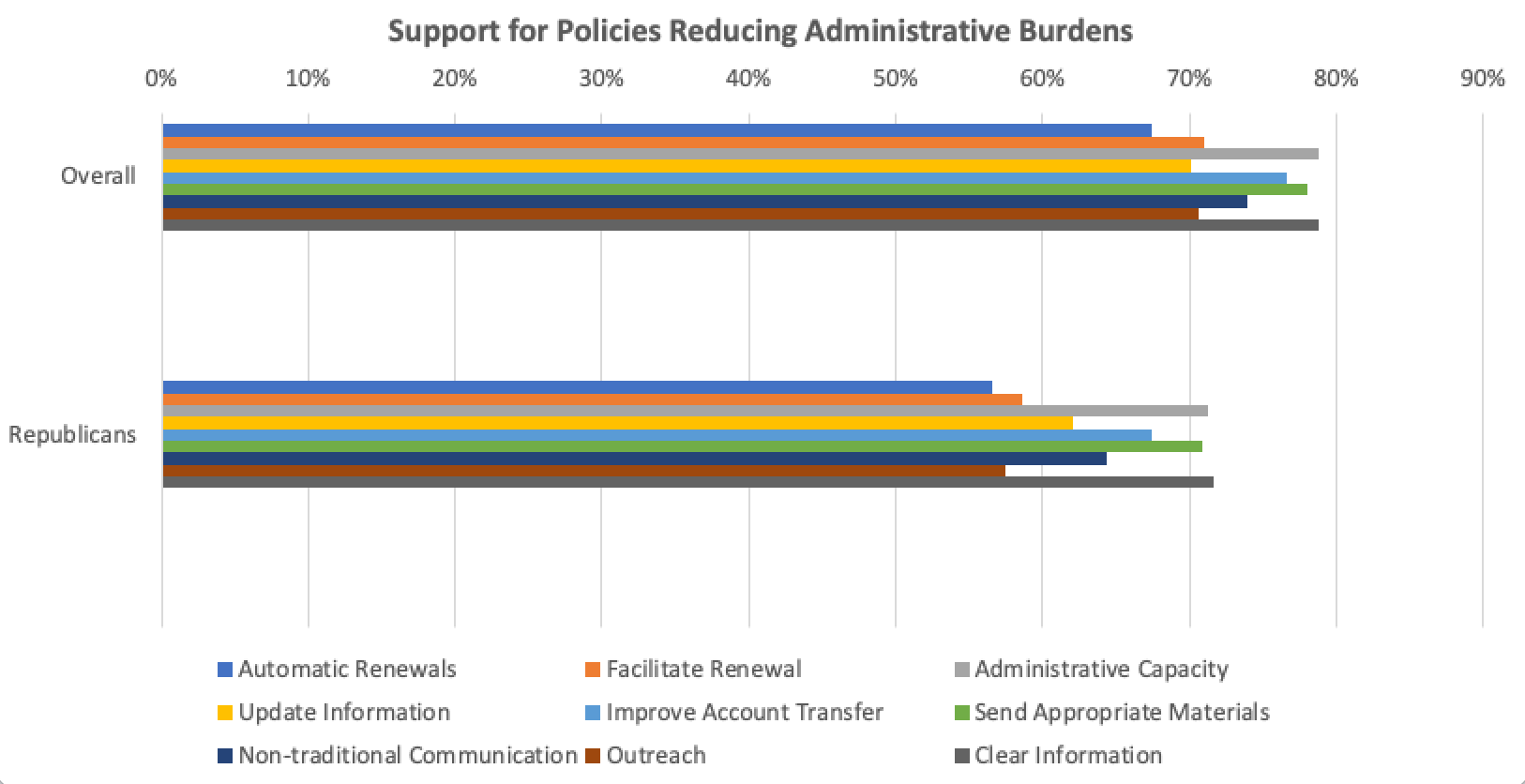
The actions we surveyed people about are feasible, evidence-based burden-reduction strategies: using administrative data to automatically enroll those who were clearly eligible, pre-filling renewal forms, updating contact information, or improving account transfer processes with Affordable Care Act marketplaces. Other policies reflected more comprehensive outreach, such as using texts and emails, plain language communication rather than bureaucratese, or hiring navigators to help enroll those who are eligible. We also asked about ensuring that states should have the administrative resources in place to manage the PHE surge.
Some states are pursuing some combination of these strategies. But they can, and should, do more. (If you want to stay on top of the Great Unwinding, and what states are actually doing, the Kaiser Family Foundation and Georgetown’s Center for Children and Families provide detailed and up-to-date information).
We found that the public was broadly supportive of administrative actions that would reduce Medicaid enrollment burdens. All of the policies had significant majority support. On average, such policies were supported by 74% of those polled. This is a remarkable level of support one rarely sees for any policy.
It is important to note that this support for action to reduce administrative burdens was bipartisan. This in the context of Republican Governors pushing President Biden to end the PHE. Red states also have a track record of creating more burdensome Medicaid processes, and saw more intense losses in coverage before the pandemic. Conservative voters and Governors are also more supportive of policies such as Medicaid work requirements.
We found that Republicans were indeed less supportive than Democrats when it comes to easing burdens. But “less supportive” does not mean “opposed.” A substantial majority of Republicans, 6 or 7 out of 10 depending on the specific policy, supported the actions to ease burdens.
Both Democrats and Republicans want government to proactively eliminate administrative hassles when they can.
We also found that those with more first-hand experience of Medicaid, those who reported struggling with burdens, and those with higher empathy and lower racial prejudice were especially likely to support the policies to reduce burdens in Medicaid. But across every demographic factor we measured – education, income, gender, race – we found strong majorities for such actions.
We should ask people about administrative burdens more
In media and policymaking circles, we talk a great deal about policy, but not enough about how it is implemented. This is a mistake, because seemingly technical details of administration may be just as important as policy design when it comes to helping people. This lack of attention may be why policy implementation is often scattershot, ineffectual, and inequitable.
But if we take the time to ask the public, we can learn a lot about their experiences and attitudes when it comes to policy implementation. Here is another example: A recent survey by the Urban Institute found that 40% of people who applied for or received safety net programs said they had trouble proving eligibility or getting benefits when they needed them.
Our survey found that people overwhelmingly want government to use the tools it can to make policies work. Maybe the results are not all that surprising. After all, it turns out that the public likes access to public health insurance, as represented by the success of Medicaid expansions, even in some very red states. So it’s not altogether surprising they want administrative processes in place to ensure that the promise of coverage is not an empty one.
The results of this survey should reassure governments who are doing all the can to maintain Medicaid coverage that the public is behind them. It should push governments who are lagging to do more. The scale of the potential loss of coverage is too big to ignore, and governments can’t say they did not see it coming. The next year will offer a very visible test of which governments want their residents to have health insurance and have the capacity to ensure they get it.
 | A guest post by
|